
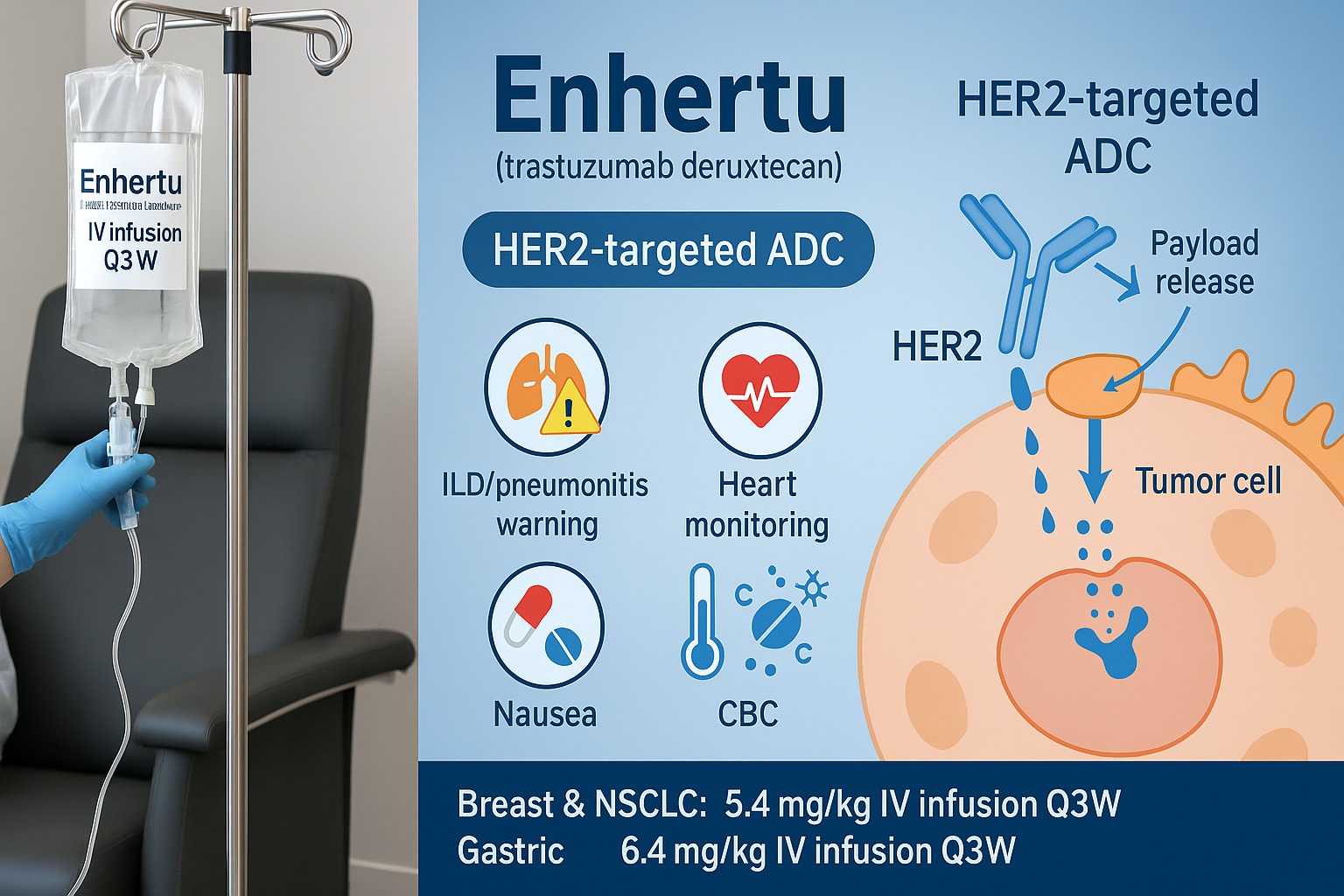
Enhertu (generic name trastuzumab deruxtecan) is a prescription antibody–drug conjugate (ADC) used in certain breast, lung, and stomach (gastric/G-E junction) cancers that express HER2. It’s given by IV infusion in a clinic. Enhertu links a HER2-targeting antibody to a potent chemotherapy payload, so it delivers treatment inside HER2-expressing cancer cells while limiting exposure to the rest of the body.
This clear, patient-friendly guide explains what Enhertu is, who it’s for, how it works, how it’s given, important side effects (including interstitial lung disease/pneumonitis), precautions, answers to top-searched questions (HER2-low, price, hair loss, nausea, heart effects, infusion time), and practical tips for safer treatment.
Quick disclaimer: This article is educational and not medical advice. Enhertu must be prescribed and monitored by experienced oncology teams. Always follow your clinician’s instructions and the Medication Guide that comes with the drug.
What Is Enhertu?
Enhertu is an antibody-drug conjugate (ADC). Think of it as a guided missile:
- The antibody part (trastuzumab) recognizes HER2 on the surface of some cancer cells.
- A linker holds multiple molecules of a chemotherapy payload (deruxtecan, a topoisomerase-I inhibitor).
- After binding to HER2, the ADC is swallowed into the cancer cell, the linker releases the chemo inside, and the cell is damaged from within. Some of the released drug can also affect nearby tumor cells, a “bystander effect,” which may help when HER2 expression is uneven.
Cancers Enhertu May Treat (Adults)
Your oncologist may consider Enhertu for one of the following FDA-/EMA-approved uses (exact wording may differ by region):
- Breast cancer
- HER2-positive metastatic or unresectable disease after prior anti-HER2 therapy.
- HER2-low (IHC 1+ or 2+/ISH–) and, in some regions, HER2-ultralow hormone receptor-positive metastatic disease after endocrine therapy and at least one line of chemotherapy, or when chemo is not appropriate.
- Non-small cell lung cancer (NSCLC)
- HER2-mutant metastatic NSCLC that has progressed on or after systemic therapy.
- Gastric or gastroesophageal junction (GEJ) adenocarcinoma
- HER2-positive disease after prior trastuzumab-based regimen.
Eligibility is based on pathology testing (immunohistochemistry/ISH for protein expression; next-generation sequencing for HER2 mutations in lung cancer). Your team will confirm whether your tumor meets criteria and whether other therapies should come first.
How Does Enhertu Work?
- Targets: The trastuzumab component finds HER2 on tumor cells.
- Delivers chemo: Inside the cell, the linker breaks, releasing deruxtecan, which inhibits topoisomerase-I, an enzyme cancer cells need to copy DNA.
- Bystander effect: The payload can diffuse into neighboring tumor cells—even those with lower HER2—potentially improving tumor kill.
- Immune effects: The antibody portion can also recruit the immune system (antibody-dependent cellular cytotoxicity), adding to anti-tumor activity.
Dosing & Administration
Your exact plan comes from your oncologist. Typical adult regimens:
- Breast cancer (most settings): 5.4 mg/kg IV infusion once every 3 weeks (Q3W).
- Gastric/GEJ cancer: 6.4 mg/kg Q3W.
- HER2-mutant NSCLC: 5.4 mg/kg Q3W.
Infusion Schedule & Time
- Cycle length: 21 days.
- First infusion: about 90 minutes with close monitoring.
- If tolerated: later infusions may run over 30 minutes.
- Premedication for nausea is common (e.g., a 2–3 drug antiemetic plan). Your team may add steroid/antihistamine if you’ve had infusion reactions.
Dose Adjustments
If certain side effects occur (e.g., interstitial lung disease/pneumonitis, low blood counts, heart issues, or severe nausea/vomiting), clinicians can hold, reduce, or stop treatment based on official criteria. Never change a dose on your own.
What to Expect on Treatment
- Before starting: labs (CBC, CMP), pregnancy test if applicable, baseline chest imaging and heart assessment (e.g., echocardiogram) per clinic protocol.
- During therapy: routine blood counts, liver tests, heart function (periodically), and symptom checks each cycle.
- Imaging scans every few cycles to measure tumor response.
Bring a list of all medications and supplements to each visit. Some drugs can raise lung or heart risks or worsen nausea.
Side Effects of Enhertu
Enhertu can cause mild to serious effects. Many are manageable with proactive care.
Common (often manageable)
- Nausea & vomiting (can be significant without strong premedication)
- Fatigue
- Low blood counts: anemia, neutropenia, thrombocytopenia
- Hair thinning/hair loss (alopecia)
- Decreased appetite, constipation or diarrhea
- Increased liver enzymes
- Cough or shortness of breath (always report promptly)
Serious but important to know
- Interstitial lung disease (ILD)/pneumonitis — the key boxed warning
- Can be fatal if missed. Tell your team immediately about new or worsening cough, shortness of breath, fever, or chest pain, even if mild.
- Management ranges from holding or discontinuing Enhertu to steroids and pulmonary consults, depending on severity.
- Cardiac dysfunction (decreased LVEF/heart failure) — less common than with some HER2 antibodies but still monitored.
- Severe myelosuppression — may raise infection or bleeding risk.
- Infusion-related reactions — fever, chills, flushing, or rash during/after infusion.
- Severe nausea/vomiting — controlled with antiemetic plans; call your clinic early for help.
- Embryo-fetal toxicity — can harm an unborn baby.
If symptoms change suddenly, call your oncology team or seek urgent care. It’s always safer to over-report than to wait.
Warnings & Precautions
- ILD/Pneumonitis: Report any breathing change immediately. Your team may order a CXR or CT scan and pulmonology review.
- Heart function: Baseline and periodic echocardiograms/MUGA may be done. New leg swelling, shortness of breath at rest, rapid weight gain, or persistent cough can signal heart issues—report promptly.
- Bone marrow suppression: Expect regular CBCs; watch for fever, sore throat, mouth sores, easy bruising, or prolonged bleeding.
- Pregnancy & contraception: Use effective birth control during therapy and for the recommended period after the last dose (your team will specify). Do not breastfeed during treatment and for a period after.
- Hepatic/renal impairment: Dosing/monitoring may be adjusted.
- Drug interactions: Tell your team about all prescription drugs, OTCs (including NSAIDs), vitamins, and herbal supplements (e.g., St. John’s wort).
- Vaccinations: Inactivated vaccines may be allowed; live vaccines are generally avoided during chemotherapy-like treatments—ask your oncologist.
Enhertu vs Other HER2-Directed Options
- Compared with trastuzumab + chemo or T-DM1: Enhertu delivers more payload per antibody and has a bystander effect, which may help in HER2-low tumors.
- Compared with small-molecule HER2 TKIs (e.g., tucatinib, neratinib): Different mechanisms and side-effect profiles; sometimes used before or after each other depending on your disease, prior therapies, and guidelines.
- In HER2-mutant lung cancer: Enhertu offers a non-TKI option after prior systemic therapy and is selected based on mutation profile and prior response.
Your team personalizes the sequence to fit your cancer type, prior treatments, side-effect tolerance, and goals.
Practical Tips to Feel Better on Enhertu
- Nausea prevention
- Take antiemetics exactly as prescribed (often a 3-drug regimen on infusion day plus several days after).
- Eat small, frequent meals; bland foods (rice, toast, bananas, crackers) can help.
- Sip fluids steadily; try ginger or peppermint if approved.
- Energy & activity
- Gentle daily movement (short walks, stretching) often reduces fatigue.
- Prioritize sleep, and plan important tasks on higher-energy days.
- Infection prevention
- Wash hands, avoid sick contacts, and call early for fever ≥38°C (100.4°F).
- Mouth & gut care
- Use alcohol-free mouthwash, soft toothbrush, and stay hydrated.
- For constipation, increase fluids and fiber; use clinic-approved remedies.
- For diarrhea, start anti-diarrheals per plan and call if persistent.
- Hair & skin
- Discuss scalp cooling (availability varies).
- Moisturize skin; use sunscreen—some treatments can increase sensitivity.
- Breath changes
- Do not ignore a new cough or shortness of breath. Call the clinic the same day—this could be ILD.
Cost, Access & “Generic” Status
- Enhertu is a brand-name specialty therapy without a true generic.
- Most patients use insurance prior authorization, and your center or the manufacturer can help with co-pay support or patient assistance programs if eligible.
- Infusion center charges (nursing, pharmacy, facility) are part of total cost; ask your team for a benefits check so you can plan.
Frequently Asked Questions (12)
1) What does “HER2-low” or “HER2-ultralow” mean?
HER2 is measured by IHC (0, 1+, 2+) and sometimes ISH. HER2-low usually means IHC 1+ or 2+/ISH-negative. Ultralow refers to very faint (IHC 0 with patchy staining) in some settings. Your pathologist’s report and current approvals determine eligibility.
2) How long will I stay on Enhertu?
You typically continue as long as it helps and side effects are manageable. Scans and clinic visits guide decisions.
3) How quickly might I feel a difference?
Some people notice symptom relief within a few weeks, but tumor response is assessed on scans every 6–12 weeks.
4) Will I lose my hair?
Hair thinning or loss can happen, though it varies by person. Ask about scalp cooling, gentle hair care, and support resources.
5) What are the early signs of ILD/pneumonitis?
New dry cough, shortness of breath, fever, fatigue, or chest discomfort—even mild—are red flags. Stop exertion and call your clinic immediately.
6) Does Enhertu affect the heart like trastuzumab?
Heart monitoring is still recommended. Tell your team about new swelling, breathlessness at rest, or rapid weight gain.
7) Can Enhertu be combined with endocrine therapy or other chemo?
Most people take it alone (monotherapy). Combinations are studied in clinical trials; outside trials, your oncologist follows current standards.
8) What if my counts are low on lab day?
Your infusion may be delayed, and doses adjusted. You might receive growth-factor support or transfusions in specific cases.
9) Can I work during treatment?
Many people do, with adjustments. Plan around infusion days and the days you typically feel fatigued. Ask your care team for work notes or schedule modifications.
10) What about fertility, pregnancy, and breastfeeding?
Enhertu can harm an unborn baby. Use effective contraception during treatment and for the recommended period after the last dose. Do not breastfeed during treatment and for a time after—confirm details with your team.
11) What should I bring to infusion day?
A snack, water bottle, warm layer, headphones, and a list of questions. Arrive a bit early for labs and vital signs.
12) Is there financial help?
Yes. Ask your center’s financial counselor and visit the manufacturer’s support site for co-pay cards and assistance programs if you qualify.
Special Section: Enhertu vs T-DM1 (Kadcyla) at a Glance
- Both are HER2-targeted ADCs.
- Enhertu carries more payload molecules and has a bystander effect; this partly explains its activity in HER2-low tumors.
- Side-effect profiles differ:
- Enhertu: higher rates of nausea and ILD risk (requires strict monitoring).
- T-DM1: more platelet drops and neuropathy in some patients.
Your oncologist chooses based on prior drugs, tumor biology, comorbidities, and current guidelines.
Proper Handling & Clinic-Day Checklist
- Enhertu is prepared and given by professionals—no home mixing.
- Keep a personal treatment journal (dose, date, side effects, questions).
- Call early for symptoms—especially breathing changes, fever, severe nausea/vomiting, or dizziness.
- Bring an updated medication list to every visit.
Final Thoughts
Enhertu (trastuzumab deruxtecan) is a targeted antibody–drug conjugate that can help people with HER2-positive, HER2-low, and certain HER2-mutant cancers when used in the right setting. When used correctly—precise pathology testing, strong nausea prevention, vigilant monitoring for ILD and heart effects, timely dose adjustments, and open communication with your oncology team—it’s generally well managed and can be highly effective.
To get the best results:
- Confirm HER2 status (and HER2 mutation for lung cancer) with an experienced pathology lab.
- Start with a clear antiemetic plan and report breathing changes immediately.
- Keep lab and imaging appointments and follow dose holds/reductions exactly as directed.
- Ask about support programs to manage costs and logistics.
- Lean on your care team, family, and support groups—you don’t have to do this alone.
Used thoughtfully, Enhertu offers a powerful, targeted option—aimed at the tumor, with safety steps to protect you.
Leave a Comment